
Neonatal/infant Hearing Loss
Ear Anatomy
The human ear consists of three parts—the outer ear, middle ear and inner ear. The ear canal of the outer ear is separated from the air-filled tympanic cavity of the middle ear by the eardrum. The middle ear contains the three small bones—the ossicles—involved in the transmission of sound, and is connected to the throat at the nasopharynx, via the pharyngeal opening of the Eustachian tube. The inner ear contains the otolith organs—the utricle and saccule—and the semicircular canals belonging to the vestibular system, as well as the cochlea of the auditory system.
Outer ear
The outer ear is the external portion of the ear and includes the fleshy visible pinna (also called the auricle), the ear canal, and the outer layer of the eardrum (also called the tympanic membrane).
The pinna consists of the curving outer rim called the helix, the inner curved rim called the antihelix, and opens into the ear canal. The tragus protrudes and partially obscures the ear canal, as does the facing antitragus. The hollow region in front of the ear canal is called the concha. The ear canal stretches for about 1 inch (2.5 cm). The first part of the canal is surrounded by cartilage, while the second part near the eardrum is surrounded by bone. This bony part is known as the auditory bulla and is formed by the tympanic part of the temporal bone. The skin surrounding the ear canal contains ceruminous and sebaceous glands that produce protective ear wax. The ear canal ends at the external surface of the eardrum.
Two sets of muscles are associated with the outer ear: the intrinsic and extrinsic muscles. In some mammals, these muscles can adjust the direction of the pinna. In humans, these muscles have little or no effect. The ear muscles are supplied by the facial nerve, which also supplies sensation to the skin of the ear itself, as well as to the external ear cavity. The great auricular nerve, auricular nerve, auriculotemporal nerve, and lesser and greater occipital nerves of the cervical plexus all supply sensation to parts of the outer ear and the surrounding skin.
The pinna consists of a single piece of elastic cartilage with a complicated relief on its inner surface and a fairly smooth configuration on its posterior surface. A tubercle, known as Darwin’s tubercle, is sometimes present, lying in the descending part of the helix and corresponding to the ear-tip of mammals. The earlobe consists of areola and adipose tissue. The symmetrical arrangement of the two ears allows for the localisation of sound. The brain accomplishes this by comparing arrival-times and intensities from each ear, in circuits located in the superior olivary complex and the trapezoid bodies which are connected via pathways to both ears.
Middle ear
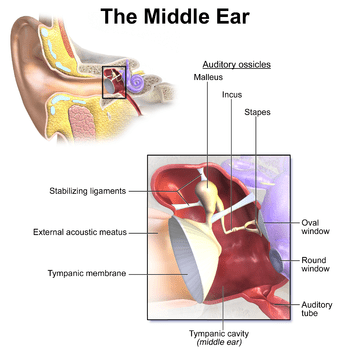 The middle ear lies between the outer ear and the inner ear. It consists of an air-filled cavity called the tympanic cavity and includes the three ossicles and their attaching ligaments; the auditory tube; and the round and oval windows. The ossicles are three small bones that function together to receive, amplify, and transmit the sound from the eardrum to the inner ear. The ossicles are the malleus (hammer), incus (anvil), and the stapes (stirrup). The stapes is the smallest named bone in the body. The middle ear also connects to the upper throat at the nasopharynx via the pharyngeal opening of the Eustachian tube.
The middle ear lies between the outer ear and the inner ear. It consists of an air-filled cavity called the tympanic cavity and includes the three ossicles and their attaching ligaments; the auditory tube; and the round and oval windows. The ossicles are three small bones that function together to receive, amplify, and transmit the sound from the eardrum to the inner ear. The ossicles are the malleus (hammer), incus (anvil), and the stapes (stirrup). The stapes is the smallest named bone in the body. The middle ear also connects to the upper throat at the nasopharynx via the pharyngeal opening of the Eustachian tube.The three ossicles transmit sound from the outer ear to the inner ear. The malleus receives vibrations from sound pressure on the eardrum, where it is connected at its longest part (the manubrium or handle) by a ligament. It transmits vibrations to the incus, which in turn transmits the vibrations to the small stapes bone. The wide base of the stapes rests on the oval window. As the stapes vibrates, vibrations are transmitted through the oval window, causing movement of fluid within the cochlea.
The round window allows for the fluid within the inner ear to move. As the stapes pushes the secondary tympanic membrane, fluid in the inner ear moves and pushes the membrane of the round window out by a corresponding amount into the middle ear. The ossicles help amplify sound waves by nearly 15–20 times.
Inner ear
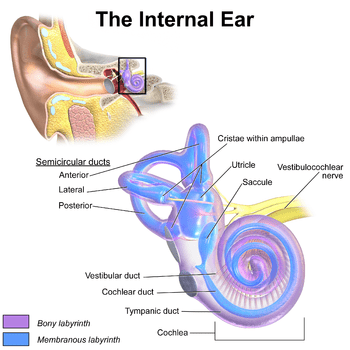
The inner ear sits within the temporal bone in a complex cavity called the bony labyrinth. A central area known as the vestibule contains two small fluid-filled recesses, the utricle and saccule. These connect to the semicircular canals and the cochlea. There are three semicircular canals angled at right angles to each other which are responsible for dynamic balance. The cochlea is a spiral shell-shaped organ responsible for the sense of hearing. These structures together create the membranous labyrinth.
The bony labyrinth refers to the bony compartment which contains the membranous labyrinth, contained within the temporal bone. The inner ear structurally begins at the oval window, which receives vibrations from the incus of the middle ear. Vibrations are transmitted into the inner ear into a fluid called endolymph, which fills the membranous labyrinth. The endolymph is situated in two vestibules, the utricle and saccule, and eventually transmits to the cochlea, a spiral-shaped structure. The cochlea consists of three fluid-filled spaces: the vestibular duct, the cochlear duct, and the tympanic duct. Hair cells responsible for transduction—changing mechanical changes into electrical stimuli are present in the organ of Corti in the cochlea.
Physiology of hearing
Sound waves travel through the outer ear, are modulated by the middle ear, and are transmitted to the vestibulocochlear nerve in the inner ear. This nerve transmits information to the temporal lobe of the brain, where it is registered as sound.
Sound that travels through the outer ear impacts on the eardrum, and causes it to vibrate. The three ossicles bones transmit this sound to a second window (the oval window) which protects the fluid-filled inner ear. In detail, the pinna of the outer ear helps to focus a sound, which impacts on the eardrum. The malleus rests on the membrane, and receives the vibration. This vibration is transmitted along the incus and stapes to the oval window. Two small muscles, the tensor tympani and stapedius, also help modulate noise. The two muscles reflexively contract to dampen excessive vibrations. Vibration of the oval window causes vibration of the endolymph within the vestibule and the cochlea.
The inner ear houses the apparatus necessary to change the vibrations transmitted from the outside world via the middle ear into signals passed along the vestibulocochlear nerve to the brain. The hollow channels of the inner ear are filled with liquid, and contain a sensory epithelium that is studded with hair cells. The microscopic “hairs” of these cells are structural protein filaments that project out into the fluid. The hair cells are mechanoreceptors that release a chemical neurotransmitter when stimulated. Sound waves moving through fluid flows against the receptor cells of the organ of Corti. The fluid pushes the filaments of individual cells; movement of the filaments causes receptor cells to become open to receive the potassium-rich endolymph. This causes the cell to depolarise, and creates an action potential that is transmitted along the spiral ganglion, which sends information through the auditory portion of the vestibulocochlear nerve to the temporal lobe of the brain.
The human ear can generally hear sounds with frequencies between 20 Hz and 20 kHz (the audio range). Sounds outside this range are considered infrasound (below 20 Hz) or ultrasound (above 20 kHz). Although hearing requires an intact and functioning auditory portion of the central nervous system as well as a working ear, human deafness (extreme insensitivity to sound) most commonly occurs because of abnormalities of the inner ear, rather than in the nerves or tracts of the central auditory system.
Development
During embryogenesis the ear develops as three distinct structures: the inner ear, the middle ear and the outer ear. Each structure originates from a different germ layer: the ectoderm, endoderm and mesenchyme.
Inner ear
Around the 33rd day of development, the vesicles begin to differentiate. Closer to the back of the embryo, they form what will become the utricle and semicircular canals. Closer to the front of the embryo, the vesicles differentiate into a rudimentary saccule, which will eventually become the saccule and cochlea. Part of the saccule will eventually give rise and connect to the cochlear duct. This duct appears approximately during the sixth week and connects to the saccule through the ductus reuniens.
As the cochlear duct’s mesenchyme begins to differentiate, three cavities are formed: the scala vestibuli, the scala tympani and the scala media. Both the scala vestibuli and the scala tympani contain an extracellular fluid called perilymph. The scala media contains endolymph. A set of membranes called the vestibular membrane and the basilar membrane develop to separate the cochlear duct from the vestibular duct and the tympanic duct, respectively.
Parts of the otic vesicle in turn form the vestibulocochlear nerve. These form bipolar neurons which supply sensation to parts of the inner ear (namely the sensory parts of the semicircular canals, macular of the utricle and saccule, and organ of Corti). The nerve begins to form around the 28th day.[16]
- Molecular regulation
Most of the genes responsible for the regulation of inner ear formation and its morphogenesis are members of the homeobox gene family such as Pax, Msx and Otx homeobox genes. The development of inner ear structures such as the cochlea is regulated by Dlx5/Dlx6, Otx1/Otx2 and Pax2, which in turn are controlled by the master gene Shh. Shh is secreted by the notochord.[19]
Middle ear
The middle ear and its components develop from the first and second pharyngeal arches. The tympanic cavity and auditory tube develop from the first part of the pharyngeal pouch between the first two arches in an area which will also go on to develop the pharynx. This develops as a structure called the tubotympanic recess. The ossicles (malleus, incus and stapes) normally appear during the first half of fetal development. The first two (malleus and incus) derive from the first pharyngeal arch and the stapes derives from the second. All three ossicles develop from the neural crest. Eventually cells from the tissue surrounding the ossicles will experience apoptosis and a new layer of endodermal epithelial will constitute the formation of the tympanic cavity wall.[15]
Outer ear
Unlike structures of the inner and middle ear, which develop from pharyngeal pouches, the ear canal originates from the dorsal portion of the first pharyngeal cleft. It is fully expanded by the end of the 18th week of development. The eardrum is made up of three layers (ectoderm, endoderm and connective tissue). The pinna originates as a fusion of six hillocks. The first three hillocks are derived from the lower part of the first pharyngeal arch and form the tragus, crus of the helix, and helix, respectively. The final three hillocks are derived from the upper part of the second pharyngeal arch and form the antihelix, antitragus, and earlobe. The outer ears develop in the lower neck. As the mandible forms they move towards their final position level with the eyes.
Clinical significance
Hearing loss
Causes of conductive hearing loss include an ear canal blocked by ear wax, ossicles that are fixed together or absent, or holes in the eardrum. Conductive hearing loss may also result from middle ear inflammation causing fluid build-up in the normally air-filled space, such as by otitis media. Tympanoplasty is the general name of the operation to repair the middle ear’s eardrum and ossicles. Grafts from muscle fascia are ordinarily used to rebuild an intact eardrum. Sometimes artificial ear bones are placed to substitute for damaged ones, or a disrupted ossicular chain is rebuilt in order to conduct sound effectively.
Hearing aids or cochlear implants may be used if the hearing loss is severe or prolonged. Hearing aids work by amplifying the sound of the local environment and are best suited to conductive hearing loss. Cochlear implants transmit the sound that is heard as if it were a nervous signal, bypassing the cochlea.
Congenital abnormalities
Anomalies and malformations of the pinna are common. These anomalies include chromosome syndromes such as ring 18. Children may also present cases of abnormal ear canals and low ear implantation. In rare cases no pinna is formed (atresia), or is extremely small (microtia). Small pinnae can develop when the auricular hillocks do not develop properly. The ear canal can fail to develop if it does not channelise properly or if there is an obstruction. Reconstructive surgery to treat hearing loss is considered as an option for children older than five, with a cosmetic surgical procedure to reduce the size or change the shape of the ear is called an otoplasty. The initial medical intervention is aimed at assessing the baby’s hearing and the condition of the ear canal, as well as the middle and inner ear. Depending on the results of tests, reconstruction of the outer ear is done in stages, with planning for any possible repairs of the rest of the ear.
Approximately one out of one thousand children suffer some type of congenital deafness related to the development of the inner ear. Inner ear congenital anomalies are related to sensorineural hearing loss and are generally diagnosed with a computed tomography (CT) scan or a magnetic resonance imaging (MRI) scan. Hearing loss problems also derive from inner ear anomalies because its development is separate from that of the middle and external ear. Middle ear anomalies can occur because of errors during head and neck development. The first pharyngeal pouch syndrome associates middle ear anomalies to the malleus and incus structures as well as to the non-differentiation of the annular stapedial ligament. Temporal bone and ear canal anomalies are also related to this structure of the ear and are known to be associated with sensorineural hearing loss and conductive hearing loss.